- Program
- Faculty
- Pricing
- Hotel & Travel
- Exhibitors & Supporters
- News & Insights
The Official Meeting of Vascular Disease Management
A patient presenting with severe chronic limb-threatening ischemia (CLTI) and extensive comorbidities required a highly strategic and adaptable endovascular approach. This case highlights how a structured, stepwise methodology can support successful outcomes in even the most complex anatomies.
Review the case below, then join Dr. John Phillips at AMP 2026 to learn more about advanced strategies for treating complex CLTI and heavily calcified disease.

Dr. John A. Phillips, MD is a cardiology and peripheral vascular interventionalist in Columbus, Ohio. He is affiliated with OhioHealth, Riverside Methodist Hospital and has been in practice there for 9 years. Dr. Phillips is the system director for the OhioHealth Vascular Institute, the medical director for endovascular medicine and the clinical operations council chief for the heart and vascular service line at Riverside Methodist.
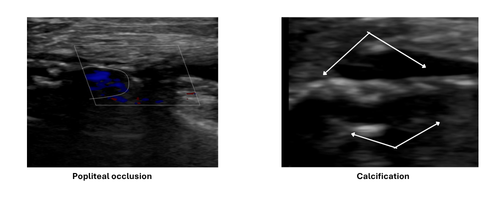
Severe calcification and total occlusion of the popliteal artery created significant barriers to lesion crossing and effective vessel preparation. Traditional crossing strategies were insufficient, requiring escalation and precise technique to establish a viable treatment pathway.
Careful imaging and duplex evaluation confirmed:
This informed the need for an advanced vessel preparation strategy.

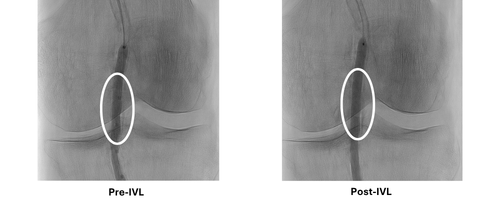
A stepwise calcium modification approach was used:
This combination enabled optimal lesion preparation prior to definitive therapy.
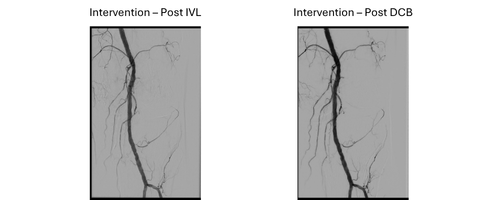
With the vessel adequately prepared:
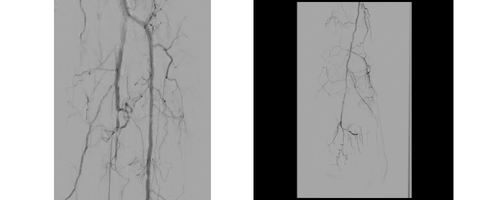
This case demonstrates the importance of:
By aligning technique with this framework, physicians can better navigate challenging lesions and optimize procedural success.
AMP in Action showcases real-world cases that demonstrate how physicians apply structured, evidence-based approaches to complex peripheral interventions—focusing on assessment, vessel preparation, and optimized treatment delivery.
As we look ahead to AMP 2026, these case-based insights reflect the types of discussions, techniques, and clinical decision-making you’ll experience at the meeting. From advanced vessel preparation strategies to managing heavily calcified disease, AMP 2026 will highlight how leading physicians are tackling today’s most challenging cases.